


All Issues
Preschool children learn about ‘happy teeth’: Nutrition program boosts dental health of Orange County migrant families
Publication Information
California Agriculture 49(2):28-32. https://doi.org/10.3733/ca.v049n02p28
Published March 01, 1995
PDF | Citation | Permissions
Abstract
With dental disease one of the top health concerns of California's migrant families, it is imperative to provide these families with information promoting good dental health. In this pilot project, migrant children and parents attended a 7-week series of lessons to examine the effect of nutrition education on dental health-related behaviors. By the program's end, at least 30% of participating families had decreased consumption of foods considered harmful to children's teeth and had increased consumption of healthy foods, such as vegetables.
Full text

The “Tooth Fairy” discusses the benefits of healthy teeth with children completing the dental health nutrition education program
One-third of the nation's migrant children live in California. In 1989, this amounted to almost 200,000 children, the majority of whom live in a world of poverty, constant mobility and cultural alienation. The most frequent health problem reported for these migrant children is dental disease.
According to a 1990 California Migrant Education needs assessment, 96% of migrant workers' children need dental care before age six, and 80% have active dental caries. Two out of every five migrant children (40%) do not see a dentist before age 17. Almost half (47%) of migrant families report having toothaches and 16% have gum disease. The majority seek treatment only for acute pain.
Earlier studies also documented incidence of dental and gum disease (the 1979 National Early Periodic Screening Diagnosis and Treatment Study and the 1984 California Guidelines for Health Services for Migrant Students). They cited reasons including: poor nutrition, no money or insurance for dental care, few bilingual dental health resources available, and migrant families' placing low priority on dental care.
The 1990 Hispanic Health and Nutrition Examination Survey studied 3,034 persons of Mexican descent living in California. It found that when families migrate to the United States, food consumption patterns change. Dinner is eaten later and many children prepare their own meals. This substantially increases the number of high-carbohydrate, cavity-producing snacks consumed by migrant children.
Recognizing the severity of the problem, UC Cooperative Extension home economists in Orange County initiated a collaborative effort to develop and pilot test a dental health nutrition education program for preschool children and their families. This demonstration project, called the Nutrition and Dental Health Preschool Program, had several objectives:
-
To examine the incidence and severity of dental health problems among children who attended Migrant Education preschool programs in the county.
-
To test the acceptance of a dental health nutrition education program by migrant families, their preschool children and the Migrant Education Program.
-
To examine the effects of the program, if any, on dental health-related behaviors of participating children and their parents.
Preparing the program
Bilingual curricula were designed for parents and their preschool children. Both lesson series' were adapted from nutrition education materials prepared by UC's Expanded Food and Nutrition Education Program (EFNEP), along with some supplemental materials. The curricula were designed to achieve the following objectives:
-
To increase participants' awareness and promote positive attitudes about good eating habits and preventing dental disease.
-
To teach participants how to improve their dental health through good dental habits and healthy food choices.
-
To identify and record changes in participants' knowledge, practices, and habits related to food choices and dental health.
The children's curriculum consisted of two 1-hour lessons presented each week for 7 weeks to three Migrant Education preschool groups in Huntington Beach. A total of 76 children participated. Typical activities, based on weekly themes, included discussion, stories, songs, puppet play, food models and food sample demonstrations, food preparation and tasting, finger-play games, cut and paste activities, videos, food-shopping play experience, mimes, and a home tooth-brushing chart. At the end of the program a family celebration was held at which a “Tooth Fairy” gave the children certificates of completion.
The children's lessons were videotaped to record activities, comments, and other indications of change in knowledge, behavior and attitudes. Some parents also participated in the children's sessions.
The parents' lessons consisted of seven 1-hour lessons, one per week, which were presented in another room at the same location as the preschool lessons. Lessons included discussions, videos, product displays and label-reading, food preparation and tasting, games, charts and handouts. A total of 45 parents enrolled and graduated from this EFNEP class.
We also administered a questionnaire to parents before and after completion of the program. Questions in the first survey related to household composition, family dental health history and practices, and food consumption patterns of parents and their preschool-aged children. The second added questions about program satisfaction.
Data was collected by analyzing these questionnaires; viewing video-tapes of the children's lessons; and by visual screening conducted by a volunteer dentist from the California Health Department's Dental Disease Program.
Profile of participants
Most of the parents (91%) were of Mexican descent, and had lived in the United States an average of 5.5 years. The majority were relatively young, ranging in age from 20 to 42, and were living in overcrowded quarters with limited resources. Household size ranged from two to nine people, with an average of five family members; about 20% were single-parent families. Families had one to three preschool children. More than half (59%) had two preschoolers although most families (82%) enrolled only one child in the program. Sixty percent of the families also had two to five school-age children. Three-fourths of the families shared their households with non-family occupants. One-third of these non-family occupants also had as many as three or four children of their own.
The Migrant Education Program was established in 1964 to provide supplemental instructional and health and welfare services for migrant students across the country. All families enrolled in the Migrant Education Preschool Program in Orange County were below U.S. poverty guidelines. The average hourly wage rate of the parents was $4.50, which amounted to an estimated monthly income of $720 for one full-time worker. The self-reported household income was about $900 per month. Three out of five families had no health insurance; only one-fifth received food stamps and Medi-Cal assistance. Most of those eligible were unaware of federal income or food assistance programs. Fifty-three percent owned a car; 35% used the bus for transportation.
Parents who enrolled their children in the program were asked about three aspects of their own and their children's dental hygiene: (1) frequency of dental examinations; (2) incidence of dental problems; and (3) frequency of brushing and flossing teeth.
Of the 45 parents who responded to a pre-program questionnaire, 60% had never had a dental examination. Only one of the remaining parents had first visited a dentist more than 5 years ago; most (17) had their first dental exam within the last 3 years. When asked how frequently they had dental exams, seven indicated they did so on a regular basis. The others reported they sought dental care only when they had a problem. Almost half (45%) of the parents reported having dental problems.
Almost all parents (91%) reported brushing their teeth once a day; the others said they brushed several times a week. Only six (13%) said they flossed daily; most (75%) had never used dental floss.
Over three-fourths (78%) of the children enrolled had never had a dental examination. The 10 parents who said they had taken their preschool children to a dentist had done so in the last year. Almost half (46%) of the parents sought treatment for their children only when something was wrong. Thirty-four percent did not know that it was important for preschool children to have dental examinations; 15% took their children to a dentist because it had been recommended, usually by an agency.
Three-fourths of the parents said they had started brushing their children's teeth before the children were 3 years old. Most children (80%) had started brushing their own teeth before they were three; some (16%) started when they were 4 or 5 years old. Four percent of the children had never brushed their teeth. About 10% of the parents used dental floss on their children's teeth.
Of the 73 children visually screened during the program, 40% needed immediate emergency care for mottled or loose teeth, dental caries or gum disease. The remaining 60% had no obvious decay, but were considered candidates for sealants.
A change in habits
Participant learning was assessed in three ways: (1) frequency of food consumption patterns of parents and children both before and after the program, (2) videotaped comments from children on how to make “happy teeth,” and (3) self-reports from parents regarding their own and their children's behavior patterns concerning dental health.
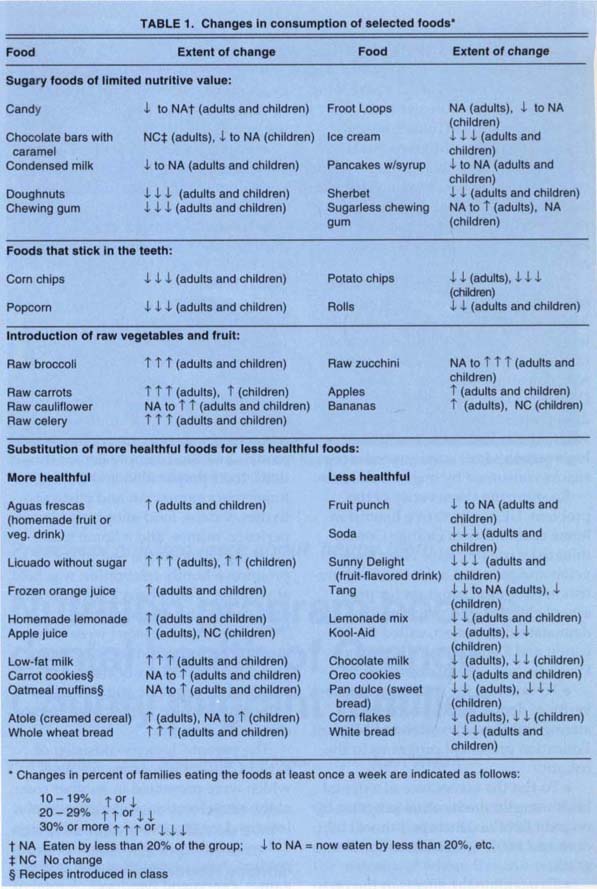
The questionnaires administered to parents before and after the program asked how often the parent and child ate the foods listed. The foods listed were selected by EFNEP nutrition educators, in collaboration with Orange County Health Department Dental Disease Program staff, for their potential impact on dental health and general nutrition. For example, sticky foods (raisins, marshmallows, caramels); sweet foods (sweet rolls, doughnuts, ice cream); and raw vegetables and fruits (celery, carrots, bananas) were included. Respondents could indicate whether they and/or their children ate the food at all, and if so, how many times per day, week, or month.
In almost all cases parents indicated that their children ate what they themselves ate, with similar frequency. In other words, if parents ate a certain food every day, so did their children. Frequency of consumption was aggregated as the proportion of respondents who reported eating a food at least once a week, and those who did not eat the food. Table 1 shows foods for which there was a change of at least 10% in the proportion of respondents who reported eating a listed food at least once a week, before and after the program had occurred.
The most remarkable changes (those in which 30% or more of parents changed their consumption of a particular food item) occurred in the decreased consumption of sugary foods with little nutritive value, such as chewing gum, fruit-flavored drinks, sodas, doughnuts, sweet rolls and ice cream. A decrease was also found for foods that stick in teeth and cause decay, such as popcorn, corn chips and potato chips. Many had begun substituting a more healthful food for a less healthful one (for example, whole wheat bread for white bread, or licuados for purchased drinks); and introducing raw vegetables and fruits, such as celery, carrots, broccoli, zucchini, apples and bananas, some of which had never been eaten by most of the respondents. At the end, 30% of the families were eating raw vegetables at least once a week.
It was not possible to compare preand post-program changes in the parents' and children's dental hygiene due to the fluctuating nature of the survey population. Often one or another parent, or another nonfamily household occupant, would participate in the program alternately. The number and names of enrolled preschool children also changed on occasion, making it impossible to match more than 18 households.
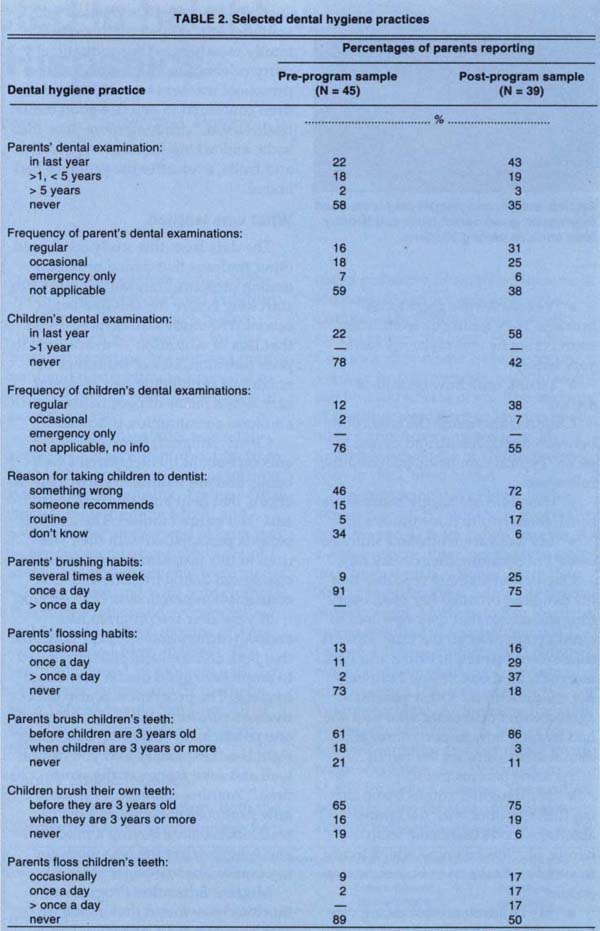
Table 2 shows the percentage of parents who reported on selected practices before and after the program was completed. In general, a larger proportion of the post-program parents reported following good dental health practices compared to those interviewed at the time of enrollment. One exception was in the parents' tooth-brushing practice, with fewer post-program parents brushing even once a day. Reported use of dental floss increased substantially for parents and children.
Some comments
Parents' reports of changes in food consumption were validated in videotaped comments from participating children. Among their many comments:
-
“I do not eat doughnuts, candy, pie, chewing gum or drink soda because it's not good for my teeth.”
-
“I'm not eating my Halloween candy. I'm giving it to the bad kids so their teeth get the cavities and mine stay healthy.”
-
“Vegetables are good tooth-brushes. They clean our teeth. They sound crunchy and make my teeth very happy.”
-
“I drink milk now instead of sodas.”

Stories, songs, and puppet play were used to promote good dental habit and healthy food choices among children.
Children also made the connection between dental health and dental hygiene. Typical comments included the following:
-
“Our teeth are happy because we brush them two to three times a day.”
-
“My teeth are white and shiny because I'm brushing them every day.”
One parent jokingly reported that his daughter brushed her teeth every time she ate, so that they now had to clean up after her all the time. Parents themselves learned to brush and floss correctly. Said one, “Now I can help my children do it.” Other parents agreed with one mother who said she had learned how important regular dental visits were for her family.
As some parents put it:
-
“My daughter comes home sharing (information) with the family about the foods that make teeth happy. She lets us know which foods to avoid and asks us to buy more vegetables.”
-
“My children are not eating candies anymore. They like to eat fruits and vegetables now and avoid candy. They are always reminding us that candy causes cavities.”
-
“The children remind us not to buy high-sugar cereals and foods while we are grocery shopping.”
Parents' attendance ranged from 18 to 31 per class; children's attendance ranged from 27 to 28. Overall response from both groups was positive. Parents not only helped with classroom activities, but invited many extended family members to the graduation party celebration. Migrant Education preschool teachers reported that children continued to practice good dental health habits, drinking more juice than soda, and asking for more vegetables and fruits, even after the program had ended.
What was learned
The data from this study confirmed other findings that dental problems among preschool migrant children can start long before the children begin school. The study also demonstrated that lack of education — in addition to poor nutrition, lack of insurance coverage and prohibitive cost of dental care — is a factor in poor dental health and food consumption practices.
Clearly, migrant farmworker parents care about their children's wellbeing, and are willing to participate in efforts that help both their children and their entire families. The fact that parents participated with their children in this program helped influence changes in dental hygiene and food consumption practices in both groups.
A year after the program had ended, teachers and site staff indicated that both children and staff continued to emphasize good dental health and hygiene. The program was also effective as a consumer education effort. As one parent said, “I learned that eating right is not expensive and you can eat well and save money at the same time.” Another reported, “I learned how to choose good juices, how to read labels before buying a product, and how to select the best foods for my family like low-sugar cereals.”
Migrant Education Program authorities have found that dental disease accounts for a substantial amount of school absenteeism, and that pain from dental disease is a serious distraction to children paying attention in school. This negative impact on learning and academic performance, with its indirect potential for eroding selfesteem, is an added burden for the children of California's migrant farmworkers. The project demonstrates that focused education can be effective, at least temporarily, in improving families' dental hygiene and nutrition. It also highlights the difficulties encountered in lining up access to dental care for treatment as well as visual screening.
The Migrant Education Program can only obtain dental care for children in pain — those requiring emergency dental work. Although many sought dental care through a California Health and Disability Prevention (CHDP) program, funding limitations did not make it possible for all who sought assistance to receive it. It was particularly disheartening, after parents had made the effort to take their children to CHDP appointments, to have some dental referrals denied because of lack of funding. The message that dental care can wait contradicts the program's emphasis on preventive care now.
Dental disease is preventable with early intervention. Dental health care is a policy issue that must be considered along with all other aspects of health care reform. Policy analysis should focus on the cost-effectiveness of alternative mixes of dental care and dental health education for all of America's children.
Although the Nutrition and Dental Health Program was designed for lowincome, Hispanic migrant families, it is suitable for any preschool setting, income level or ethnic group.
Preschool children learn about ‘happy teeth’: Nutrition program boosts dental health of Orange County migrant families

