


All Issues
In-home treatment of child abuse: Healing at home can be effective and cost-effective
Publication Information
California Agriculture 48(7):36-38.
Published December 01, 1994
PDF | Citation | Permissions
Abstract
Child abuse is an enormous and complex problem, affecting almost 3 million children in the United States. Research has shown that abused children often become abusive parents. It is therefore imperative that we treat both the abused and the abuser, to stop the cycle before it repeats itself. It is ideal to keep the child in the family, if his or her safety can be assured. But this is not always possible. This research focuses on efforts to use intensive in-home therapy in an effort to treat both the child and the abusing family, and so prevent placement in foster care, usually the next step in abusive situations.
Full text
As newspaper accounts and statistics make clear, the number of reported child abuse cases in the United States is on the rise. In 1992 alone, 2.7 million children were referred to Child Protective Services as suspected cases of abuse and neglect, according to the 1992 Children's Defense Fund Report. Although one can argue that there are problems with the way statistics are collected and interpreted, there is no doubt that America faces an enormous problem with child abuse.
The problem does not stop with the abused child. Research has shown that child abuse is cyclical: the abused child often becomes an abusing parent, as reported by John Van deKamp in 1991, when he was the state's attorney general. Because of the magnitude of the problem, much effort has been directed at treating both the abused and the abuser. The central hope behind these efforts is to break the cycle.
In this study, we have used a relatively new approach to treating child abuse through an intensive in-home treatment program that concentrates on reducing stress and increasing communication skills. The following is a short description of the program, the families involved and a summary of our findings.
The families
The target population was children in Sacramento, Yolo and Solano counties who had been referred to Child Protective Services for abuse or neglect. We selected 150 of these families and their children: half were part of the contrast group and half became part of the treatment/experimental groups. Both groups were similar in need, consisting of families in which the imminent removal of the abused child was halted only by their agreement to participate in the program. Families in the experimental group were referred to Families First, an organization structured after the Homebuilders model developed by Kinney et al. in 1976, which provides intensive in-home therapy along with traditional social services.
The contrast group, which also had been referred by Child Protective Services, agreed to receive traditional county services instead of in-home therapy. These services ideally include counseling, special tutoring as needed, and referrals to other agencies. But because of large caseloads, social workers were not always able to provide complete services to each family.
Procedure
Treatment description
Therapists were trained by Families First in family systems therapy, which addresses not just the abused child, but all family members and the family structure presumed to enable the situation to continue. The program lasted 11 months. Each therapist was assigned two families per month, working intensively with each child and his/her family from 4 to 6 weeks. Therapists were available to the families day and night, 7 days a week. Treatment was tailored to the needs of the individual child and other family members. A first step was to structure the family home situation to preclude further abuse. To do this, the therapist used a variety of methods to assess family strengths and weaknesses, provide advocacy and support in meeting basic needs, and coordinate other eligible services, such as supplemental food or income programs. As the meetings progressed, the therapist also provided training in parenting skills, mood management, and communication skills; family and individual counseling were also provided, and therapists referred clients for follow-up care as needed.
Evaluation description
Families were administered two self-report measures in an effort to evaluate whether their communication skills did improve, and stress did decrease more in the in-home therapy group than the control group.
The first — called FACES II, or the Family Adaptability and Cohesion Evaluation Scales — is used to measure the dynamics of family interactions. These dynamics can include critical areas of family interaction such as Togetherness, Child Input, Family Chaos vs. Unity, Shared Responsibilities, Difficulty in Rule Changing, and Assertiveness. The FACES II scale was administered to mothers in both groups three times: during the first week of treatment, 3 months after the therapy had ended, and at a 1-year follow-up.
Another questionnaire — called FILE or Family Inventory of Life Events — was given simultaneously. This scale is used to measure 10 dimensions of stress (McCubbin, et al., 1980). These measures include: (1) trouble with teenagers; (2) separation involving violence; (3) legal violations, such as family members in trouble with the law; (4) work; (5) family loss, through death or divorce; (6) financial strain; (7) illness and family care strain; (8) public assistance; (9) other major changes in family situation; and (10) young child management focus.
In addition to the psychological aspects of stress and communication, we examined two other variables related to the cost-effectiveness of in-home therapy: 1) Was the child still with the family at the end of the year; and 2) What was the cost of any out-of-the home placement?
Summary of findings
Stress reduction
Both the experimental and contrast groups showed reduction in stress over time. Analyses showed that overall stress could be reduced significantly in abusive families but the reduction was not associated exclusively with in-home family therapy.
Some kinds of stress were reduced more than others. Areas showing the most improvement included: trouble with teenagers, violence and separation, legal violations, work, financial strains and family illness and care strains. These results justified per forming analyses on both global and specific measures of stress (main reference: Barton, Baglio & Braverman, 1994).
Improvements in communication
In this case, the experimental group showed greater improvement than the contrast group, as well as improvement over earlier scores. Families receiving the in-home therapy, as opposed to usual social services, improved more in the following areas:
-
Chaos versus Unity. This dimension is intended to reflect how clear rules are and how, and if, family decisions are carried out by all family members. The in-home therapy group showed improvement in its scores and over the control group at both 3-month and 1-year intervals. This improvement may be attributed to the emphasis in family systems therapy on immediate crisis reduction by opening up communication channels between family members, and teaching effective communication skills such as non-hostile speech, empathic listening, and so on.
-
Shared responsibility and opinions. Here the treatment group improved significantly over the comparison group at 3 months, but no significant difference was observed between the two groups at 1 year.
-
Difficulty in rule-changing. Here, the treatment group demonstrated less difficulty in rule-changing than did the contrast group at the 1-year mark. This may reflect a newfound flexibility in dealing with problems and rules in a family.
-
Assertiveness. The treatment group showed improvement in both its initial scores and when measured against the control group at 3 months and 1 year. This improvement reflects one of the therapist's key goals in inhome therapy, which is to create an environment in which it is safe to express oneself. Verbal communication was stressed over physical expression as an appropriate way to release emotions.
-
Total family dynamics. Total family dynamics include all six factors and reflects an overall improvement in general communication skills, as reported by the author and J.L. Mullin in 1993.
Past research regarding the treatment of abused children and their families:
-
Success is maximized when treatment is given at as young an age as possible and is given in the most homelike environment. The best prognosis for a healthy future for abused infants is adoption at an early age rather than an extended stay in foster care or return to their biological families. Cautious optimism characterizes the research literature: results are best when the child is young and placement is with a family experiencing minimal stress and having the capacity to provide satisfactory parenting.
-
Treating older children is often more difficult because the abuse has continued for a longer period of time. However, the most positive treatment outcomes can be found when the treatment period has a duration of between 7 and 18 months and treatment is provided by volunteers and lay service providers. Overall, in about 20% of cases treatment will fail (i.e., child cannot be returned to the abusing home); in 40% of cases, parents will change their parenting behavior; and in 40% of cases, parents may curtail their physical abuse, but they will continue to be emotional maltreators.
-
Poor communication skills and high family stress levels have been found to be key factors in an abusive parent/child relationship. Some stressors associated with abusive episodes include intensified parent-child or parent-parent relationships, job stress, illness, financial problems and housing problems. Other related factors are gender, years married, family relationships and numbers of children. Parental history, attitudes toward child rearing, psychosis and personality variables have also been related to abuse.
-
More information can be found in studies by the following authors: Larsen, et al. (1986), Elmer (1986), Cohn & Daro (1987), Acton & During, (1990), Christopoulos, et al. (1988), Coster, et al. (1989), Crittenden (1988), Harvey, et al. (1991), Kavanagh, et al. (1988), Pearl (1988), Silber (1990), Justice & Duncan (1976), Straus (1979), Gil (1969) and Spinetta & Rigler (1972).
Cost effectiveness
An analysis of costs to the State of California indicated that in-home therapy is highly cost-effective when compared to the costs of out-of-home foster placement, which is often the end result for abusive families. The cost of placing a child in foster care was estimated at $7,200 per child. In-home therapy treatment, including the cost of the therapy for the 4- to 6-week period, on the other hand, was $5,000 per child (fig. 1, page 37). A significantly greater number of children from the experimental group were still in their homes at the 1-year follow-up (fig. 2.). The rate of foster care placement for children in the experimental group was 30% compared to 65% for the contrast group. (Main reference: Wood, Barton & Schoeder).
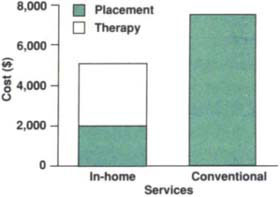
Fig. 1. The cost per family of in-home versus conventional services is depicted above. It cost the state $2,200 less to provide successful intensive in-home therapy than it did to provide traditional therapy which ended in placement of the child in a foster home. Placement costs for in-home therapy were also significantly lower.
Stress levels and family dynamics
Analyses indicate there is a significant and large interaction between stress levels and family dynamic variables. For example, when families are divided into groups with high, medium and low stress, the family dynamics variables were most healthy in the low-stress families and most dysfunctional in the high-stress families.
Directions for future research
Given the possibilities for success, it is important to ask whether the same positive effects could be achieved using less highly trained, and consequently less expensive, therapists to reach a larger number of families? Could a group of well-trained “lay” workers or regular social workers be trained in stress reduction and family systems therapy to achieve comparable results? The idea is attractive. As the population of abusing families increases, it is increasingly hard to find adequate funding to treat the families. While in-home therapy may be cost effective, the fact is there still is not enough money in the state to make it available to the whole population of abusing families.
However, before we can conclude that lay therapists can be used as effectively, it is necessary to demonstrate the degree to which these workers can measure up and under what circumstances. We have proposed a new study to explore the potential for using lay therapists successfully and to examine the concomitant cost effectiveness.

Fig. 2. Children still at home one year later as a function of in-home therapy vs. conventional treatment. Children whose families received intensive in-home therapy did not require outside placement at the rate of those in the conventional group, who received only traditional counseling services.
Future researchers should be guided by several key lessons learned through past research. They include the following:
-
Treatment should be applied as soon as possible and involve the whole family rather than individual members.
-
Treatment should be long enough (7 to 18 months for traditional therapy, or 6 to 8 weeks for intensive in-home therapy). But there seems to be no benefit to extensions over this time.
-
Treatment should be in-home, with the therapist visiting the family rather than expecting the family to come to an office. Such a set-up results in far fewer cancellations, a much better assessment of the home environment, a greater appreciation of the help received, and a much more reallife, naturalistic approach than that obtained in the therapist's office.
-
Stress reduction should be an integral part of any treatment.
-
As with stress measures, family dynamic dimensions may be useful indicators of the efficacy of treatment. The Family Adaptation and Cohesion Scales (FACES) have already been demonstrated as useful for an abusing population, and have been adapted to measure some six family dynamics dimensions as well as the traditional Adaptation and Cohesion descriptions.
-
Retention of the abused child in the family is an important goal if the safety of the child is not compromised. Our research has shown that high stress levels and poor showing on several of the family dynamics variables have been shown to predict failure to retain the child in home.
-
To ensure its future use, it is vital to examine the cost-effectiveness of any treatment. To do so, it is necessary to collect actual costs of placing children outside the home. In the past, these estimates have often been of doubtful validity. Recent research has shown that actual costs can be obtained to give studies greater credibility.
-
There is evidence that lay therapists (i.e., groups of trained volunteers) can be used effectively with child-abusing families. The next step is to design a project to assess the efficiency of such a model and provide an operational definition of the curriculum to be used in training volunteers.
-
The outcome of any treatment design cannot be assessed without considering attributes of the target population involved. People with different personalities, motivation, and ethnic backgrounds, for instance, will react differently to different types of treatment.
In conclusion, in-home treatment of child-abusing families has been shown to be more effective in retaining children in their own homes, but this goal should only be considered when the child's safety can be assured. If the cost of in-home therapy can be reduced while retaining its effectiveness, this might be a more effective way to use the limited funding available to serve a greater number of people. We must continue to try reaching abusing families with effective programs, if society is ever to address the human blight of child abuse and its consequences for future generations.
In-home treatment of child abuse: Healing at home can be effective and cost-effective

